Tackling ITB Tension: A Myotherapist’s Guide to Relief and Recovery
Tackling ITB Tension: A Myotherapist’s Guide to Relief and Recovery
Author: Jerry Song
The iliotibial band (ITB) is a crucial structure in the human body, particularly for maintaining stability during movement. However, it’s also notorious for causing discomfort and tightness, particularly among athletes and those with certain lifestyle habits.
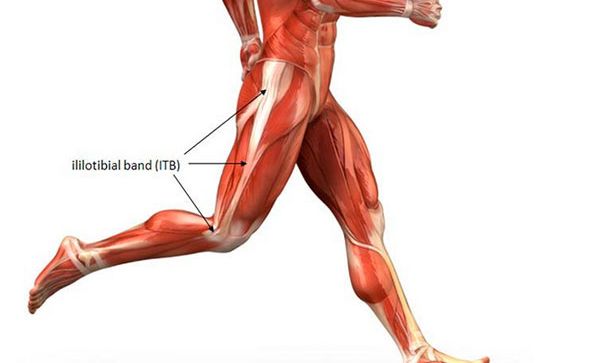
The ITB is a thick band of connective tissue that runs along the outside of the thigh. It originates at the iliac crest (hip bone) and extends down to attach to the lateral condyle of the tibia (outer side of the shinbone), just below the knee.
While the ITB itself is not a muscle, it is closely associated with the tensor fasciae latae (TFL) and the gluteus maximus muscles, which influence its tension and function.
Function of the Iliotibial Band
The ITB plays several critical roles in movement and stability:
- Lateral Stability: It stabilises the knee joint during weight-bearing activities, such as walking, running, or jumping.
- Force Transmission: The ITB helps transfer force from the hip to the lower leg, allowing for efficient movement.
- Support During Flexion and Extension: It works alongside the quadriceps and hamstrings to maintain proper alignment of the knee during flexion and extension.

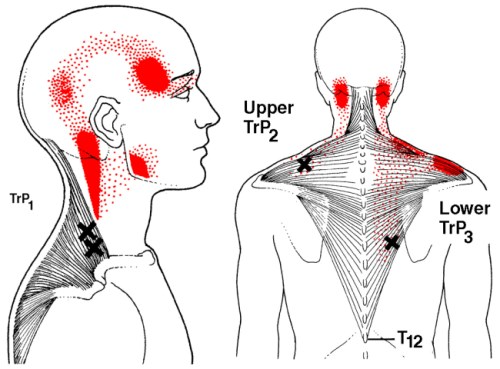
Common Trigger Points and Pain Points
Although the ITB itself doesn’t develop trigger points (as it is connective tissue and not a muscle), the muscles that interact with the ITB can develop painful trigger points that contribute to ITB tightness and dysfunction.
Key Areas of Trigger Points:
- Tensor Fasciae Latae (TFL): Trigger points in this muscle can cause tension along the ITB, resulting in pain on the outer thigh or hip.
- Gluteus Maximus and Medius: These muscles influence the ITB, and tightness or trigger points here can contribute to ITB issues.
- Vastus Lateralis (Outer Quadriceps): Trigger points in this muscle can cause referred pain along the ITB and increase tension on the band.
Pain Patterns and Symptoms:
- Pain along the outside of the thigh, particularly near the knee.
- Tenderness or tightness that worsens with activity, such as running or cycling.
- A “snapping” sensation at the hip or knee during movement.

Who Is Most Susceptible to ITB Issues?
Several demographics and activities make individuals more prone to ITB-related discomfort:
- Runners and Cyclists
- Repetitive knee flexion and extension can irritate the ITB, leading to IT Band Syndrome (ITBS).
- Athletes in Lateral Sports
- Sports requiring frequent side-to-side movements, such as tennis or soccer, place stress on the ITB.
- Desk Workers and Sedentary Individuals
- Prolonged sitting tightens the TFL and hip flexors, indirectly increasing ITB tension.
- Those with Poor Biomechanics
- Factors like overpronation, leg length discrepancies, or weak hip muscles can contribute to ITB dysfunction.
- Women
- Women may be more prone to ITB issues due to a wider pelvic structure (increased Q-angle), which can place additional stress on the ITB
Myotherapy Treatments for the Iliotibial Band
Myotherapy provides a holistic approach to treating ITB issues, focusing on both the band itself and the surrounding structures.
- Trigger Point Therapy
- Directly addressing trigger points in the TFL, gluteals, and vastus lateralis can reduce tension and alleviate pain.
- Myofascial Release
- Techniques that target the ITB and its associated muscles can improve mobility and reduce tightness.
- Dry Needling
- Inserting fine needles into the TFL, gluteals, or vastus lateralis can release deep-seated tension and restore function.
- Stretching and Mobility Exercises
- Stretching the TFL, glutes, and quadriceps can improve flexibility and reduce ITB tension.
- Example: The figure-four stretch or standing lateral stretch are effective options.
- Foam Rolling
- Care should be taken to avoid excessive pressure directly on the band. Rolling the muscles around it (e.g., TFL and quads) is often more beneficial.
- Strengthening Exercises
- Strengthening the gluteus medius and other hip stabilisers can address imbalances and reduce stress on the ITB.
- Postural and Gait Assessment
- Myotherapists can identify biomechanical issues, such as overpronation or pelvic tilt, and provide corrective exercises or orthotics advice.
- Heat and Ice Therapy
- Heat can relax tight muscles before treatment, while ice can reduce inflammation after intense activity.

Tips for Preventing ITB Tightness
Adopting these strategies can help minimise the risk of ITB issues:
- Incorporate Stretching and Strengthening: Focus on hip and thigh flexibility and stability.
- Warm-Up Properly: Always warm up before engaging in physical activities.
- Maintain Good Form: Whether running, cycling, or lifting weights, proper technique is crucial to avoid overloading the ITB.
- Use Proper Footwear: Shoes with good support can prevent biomechanical issues that contribute to ITB pain.
- Seek Regular Myotherapy: Preventative treatments can help manage tension before it develops into pain.
The iliotibial band is an essential component of lower body stability and movement, but it’s often a source of discomfort due to overuse, poor biomechanics, or lifestyle factors. While ITB tightness and pain are common, they are manageable with the right approach. Even though we’ve focused on the ITB in this article, it’s also important to note that in most cases, pain arises from multiple contributing factors, including other muscles, joints, and overall movement patterns. For this reason, it’s always best to seek a proper assessment from an experienced therapist to identify the root cause of the issue and develop an effective treatment and self-care plan.
If you or someone you know are dealing with a ITB condition, musculoskeletal pain, or even myofascial trigger points, book an appointment to see Jerry now for an initial consultation so we can assess your condition and come up with an appropriate and tailored treatment plan to manage your pain. Simply click this booking link for the myotherapy initial consultation with our experienced myotherapists.





 .
. 







































































